
The cornerstone of effective occupational therapy practice lies in meticulous record-keeping. Accurate and comprehensive progress notes are not simply documents; they are vital tools for tracking a patient’s progress, identifying areas for improvement, and informing treatment planning. A well-structured occupational therapy progress note template provides a standardized framework for capturing key information, ensuring consistency and facilitating communication among therapists, caregivers, and other healthcare professionals. This article will delve into the essential components of a robust progress note template, exploring its importance, key elements, and best practices for effective documentation. Occupational Therapy Progress Note Template – understanding and utilizing this template effectively is crucial for optimizing patient outcomes and demonstrating the value of occupational therapy.
The Importance of Progress Notes
Progress notes are far more than just a summary of what a patient did during a session. They are a dynamic record of a patient’s journey, reflecting their goals, challenges, and the interventions implemented to support their progress. They provide a chronological account of the patient’s experience, allowing for a clear understanding of how the therapy has impacted their daily life and abilities. Regularly updated progress notes are essential for monitoring changes, adjusting treatment plans, and demonstrating the effectiveness of the therapy. Without them, it becomes difficult to accurately assess the patient’s progress and ensure that the therapy remains relevant and beneficial. Furthermore, they serve as a valuable tool for legal and insurance purposes, documenting the rationale behind treatment decisions. A clear and detailed progress note can significantly streamline communication and collaboration, leading to improved patient care.
Core Components of an Occupational Therapy Progress Note
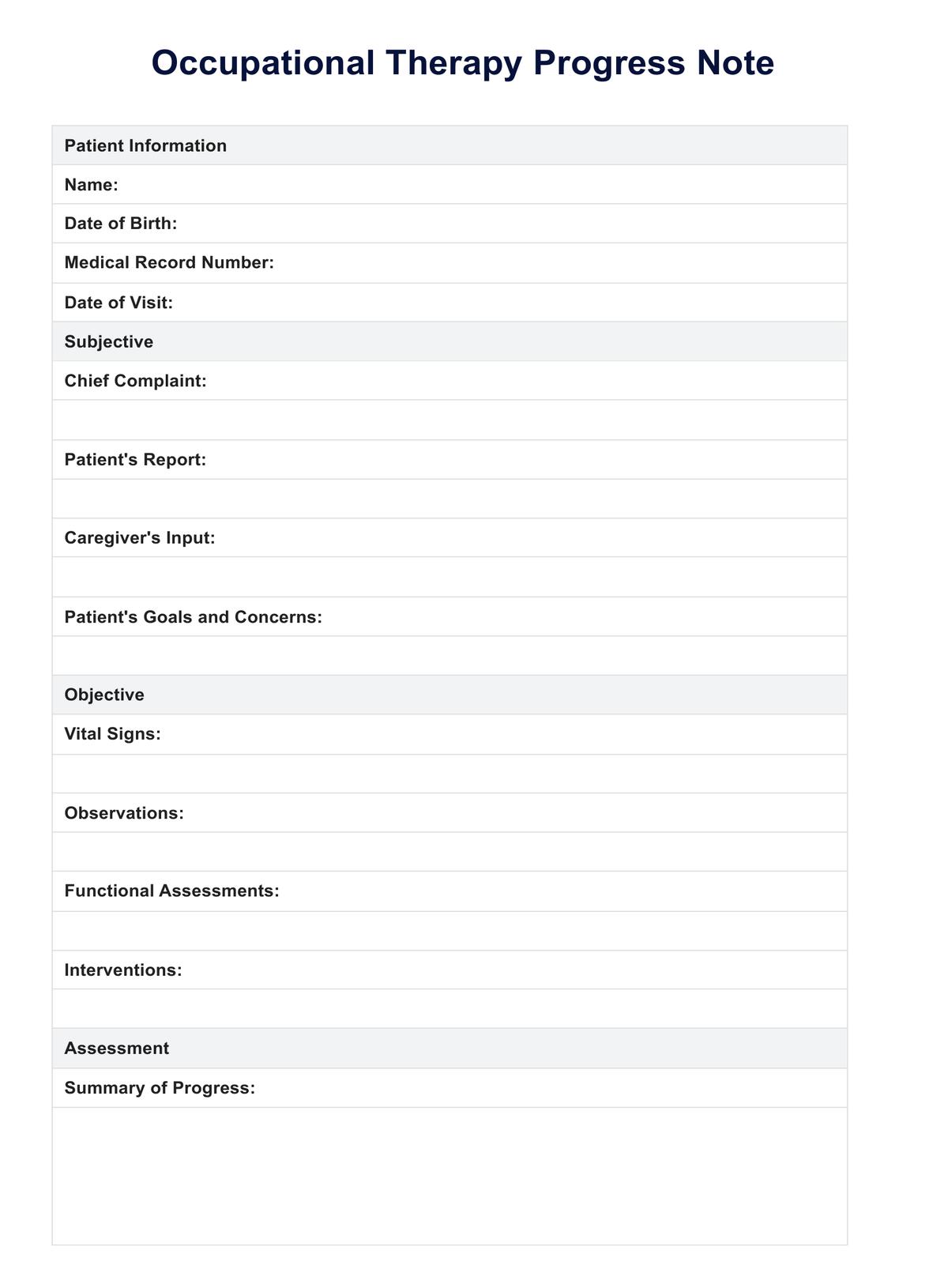
A comprehensive progress note typically includes several key sections. Each section is designed to gather specific information relevant to the patient’s current status. Here’s a breakdown of the essential elements:

1. Patient Demographics & Date
The initial section of the note should include the patient’s full name, date of birth, and contact information. The date the note was created is also crucial for tracking trends and establishing a timeline. This foundational information allows for easy identification and retrieval of the patient’s record.
2. Initial Assessment & Goals
This section summarizes the patient’s initial assessment, including any relevant medical history, functional limitations, and psychosocial factors. It also clearly outlines the patient’s initial goals, often stated as SMART (Specific, Measurable, Achievable, Relevant, Time-bound) goals. It’s important to document the reason for the initial assessment – what were the key observations that led to the initial evaluation?

3. Treatment Activities & Interventions
This is arguably the most detailed section of the note. It outlines the specific occupational therapy interventions implemented during the session. This includes describing the activities performed, the duration of each activity, and the patient’s response to the interventions. For example, instead of simply stating “assisted with dressing,” the note should detail “assisted with dressing a 7-year-old with a shirt, using a toileting aid and providing verbal cues.” It’s vital to document how the intervention was delivered and the patient’s engagement.
4. Patient Response & Progress
This section is where the real value of the progress note lies. It meticulously documents the patient’s response to the interventions. This could include observations about their ability to perform tasks, changes in their functional abilities, and any challenges they encountered. It’s important to note both positive and negative responses, as well as any areas of improvement or regression. Using a rating scale (e.g., 1-5) can provide a quantifiable measure of progress.

5. Challenges & Barriers
Identifying and documenting challenges the patient faces is crucial for tailoring treatment plans. This section should outline any obstacles preventing the patient from achieving their goals, such as difficulties with motivation, sensory sensitivities, or environmental factors. Understanding these barriers allows for proactive interventions to address them.
6. Plan & Next Steps
Finally, the note should clearly outline the plan for the next session, including specific goals, interventions, and materials to be used. It should also specify any follow-up assessments or observations that will be made. This section ensures that the patient’s progress is continuously monitored and that the treatment plan remains aligned with their needs.

Utilizing the Keyword: Occupational Therapy Progress Note Template
The keyword “Occupational Therapy Progress Note Template” is central to this document. The template itself is a critical component of effective documentation. It provides a structured framework, ensuring that all necessary information is captured consistently. Different templates exist, but the core elements outlined above – patient demographics, initial assessment, treatment activities, patient response, challenges, and plan – are universally applicable. The template should be adaptable to the specific needs of each patient and the nature of their therapy. Furthermore, utilizing a standardized template promotes efficiency and reduces the risk of omissions or inconsistencies in documentation.

Best Practices for Effective Progress Notes
Creating truly effective progress notes requires more than just filling out a form. Here are some best practices:

- Be Concise and Clear: Avoid jargon and unnecessary detail. Focus on conveying the essential information in a clear and concise manner.
- Use Precise Language: Employ specific and descriptive language to accurately portray the patient’s experience.
- Document Observations: Go beyond simply stating what the patient did. Describe how they did it and what you observed.
- Quantify Progress (When Possible): Use rating scales or numerical data to track progress whenever feasible.
- Maintain a Timely Record: Complete progress notes promptly after each session to ensure that the information is current and relevant.
- Review and Revise: Regularly review and revise progress notes to ensure accuracy and completeness.
Conclusion
Occupational Therapy Progress Note Templates are an indispensable tool for occupational therapists. They provide a structured framework for documenting patient progress, facilitating communication, and informing treatment planning. By understanding the core components of a well-written progress note and adhering to best practices, therapists can ensure that their documentation is accurate, comprehensive, and ultimately contributes to improved patient outcomes. The consistent use of this template, coupled with a commitment to detailed observation and thoughtful documentation, is paramount to the success of occupational therapy practice. Ultimately, a robust progress note serves as a vital link between the therapist and the patient, fostering a collaborative and supportive therapeutic relationship.
Additional Sections (Optional – can be expanded upon)
- Sample Progress Note (Illustrative) – A short, illustrative example demonstrating the structure and content of a progress note.
- Technology Integration – How digital progress note systems are improving the process.
- Legal Considerations – Brief overview of legal requirements for documentation.



