Mental health is a critical aspect of overall well-being, and effective communication is paramount when addressing it. A well-structured progress note can significantly improve patient care, streamline workflows, and foster stronger relationships between healthcare providers and individuals experiencing mental health challenges. This article will explore the essential components of a comprehensive progress note template specifically tailored for mental health patients, offering guidance on how to effectively document observations, interventions, and progress. Progress Note Template Mental Health is more than just a record; it’s a tool for proactive care and improved outcomes. Understanding the nuances of this template is vital for ensuring accurate and timely information.
The process of documenting mental health care can be complex, requiring a delicate balance between clinical observation and patient-centered communication. A thoughtfully crafted progress note provides a clear and concise record of the patient’s condition, treatment plan, and response to interventions. It’s a crucial element in coordinating care, identifying potential risks, and ensuring continuity of service. Furthermore, it allows for retrospective analysis to refine treatment strategies and improve patient outcomes. Effective use of this template contributes to a more holistic and responsive healthcare experience.
Understanding the Core Components of a Mental Health Progress Note
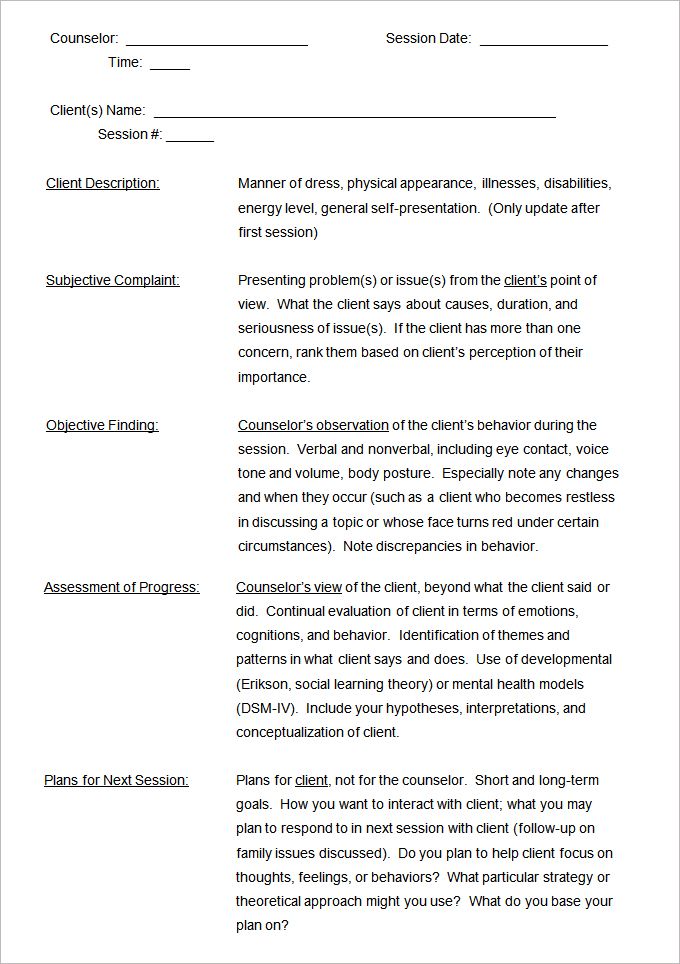
Before diving into the specific sections, it’s important to recognize the core elements that should be included in each progress note. These elements are designed to provide a complete picture of the patient’s experience and progress. A standard template typically includes:
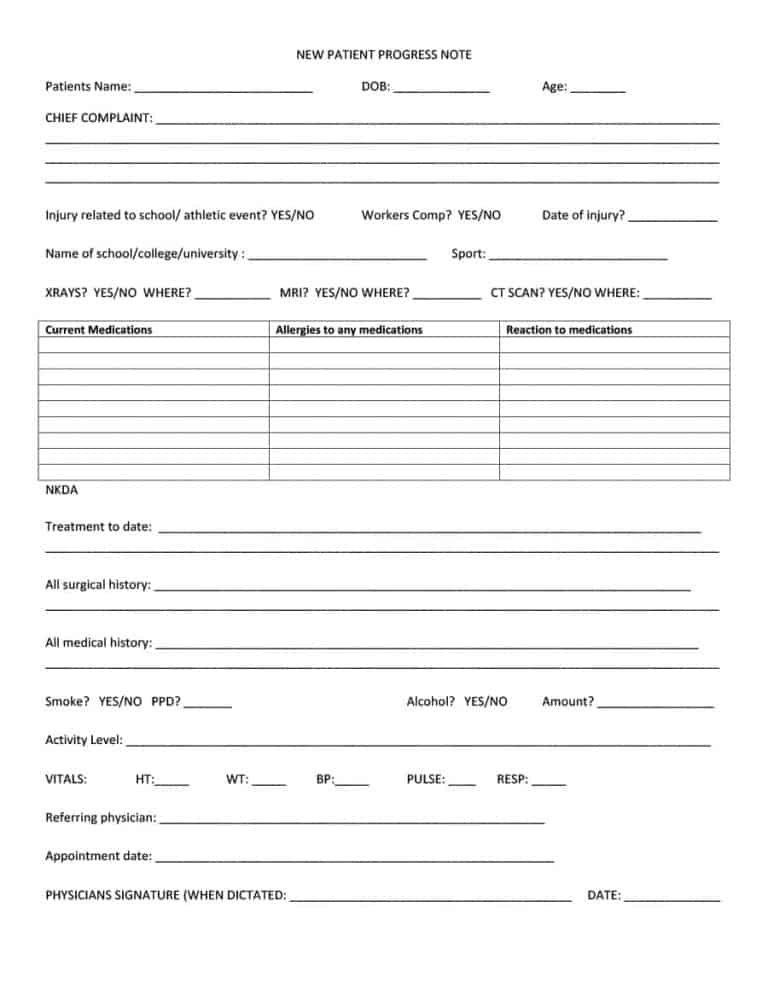
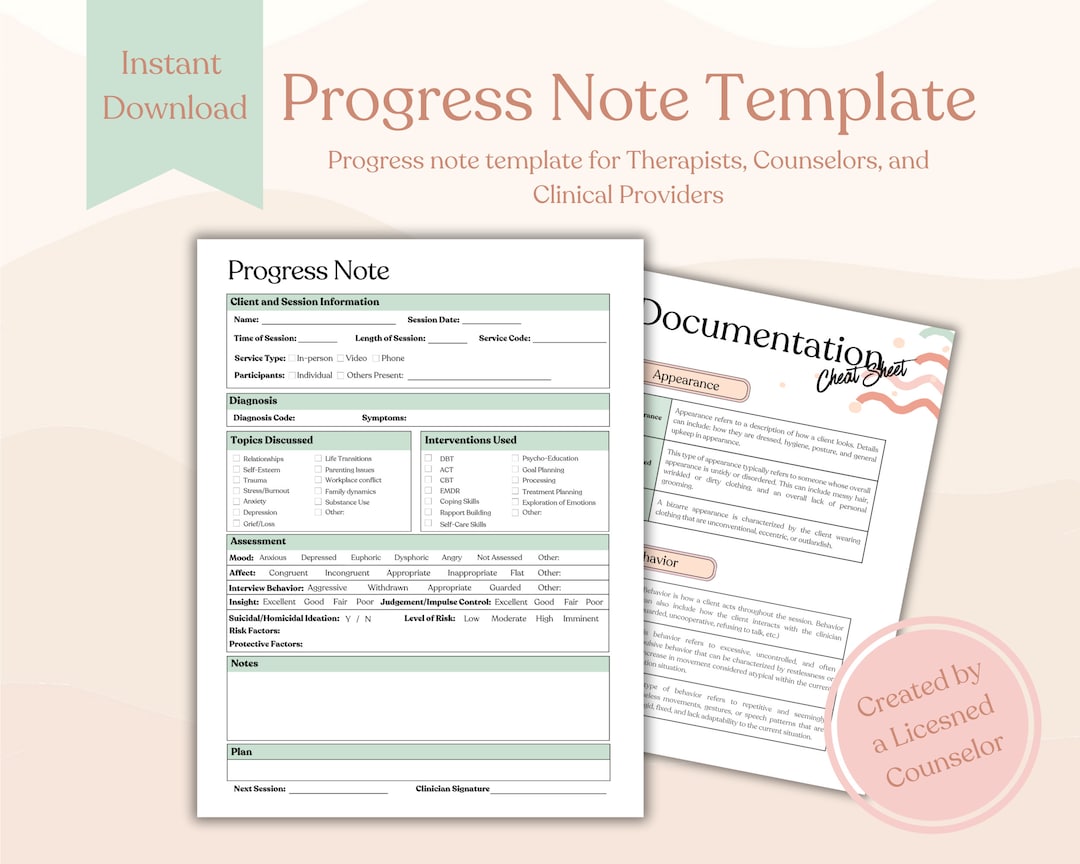
- Patient Demographics: Name, date of birth, contact information.
- Date and Time of Note: Essential for tracking the timeline of events.
- Chief Complaint: The patient’s primary reason for seeking care.
- History of Present Illness (HPI): A detailed account of the patient’s current symptoms, including onset, duration, severity, and any contributing factors. This section should be thorough and chronological.
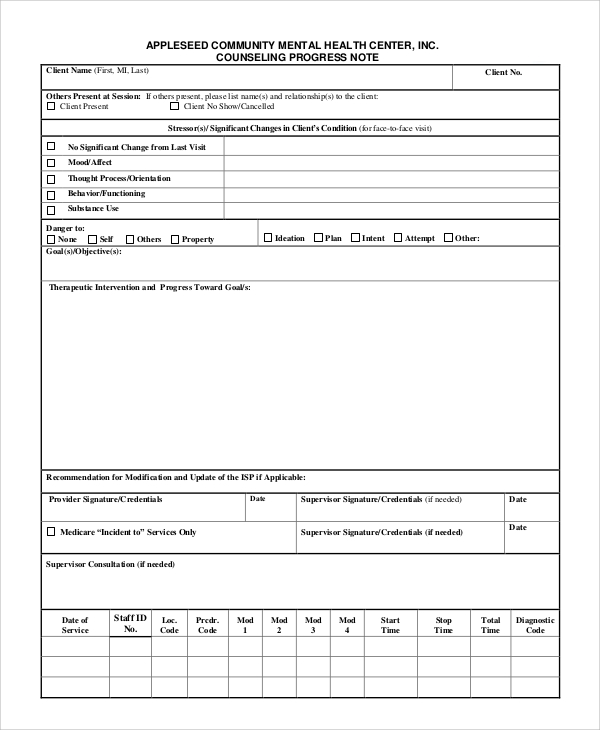
- Mental Status Examination (MSE) Findings: Observations regarding the patient’s cognitive, emotional, and behavioral state. This includes assessing their level of alertness, orientation, affect, thought processes, and compliance.
- Diagnostic Impressions: The clinician’s assessment of the patient’s diagnosis or mental health condition.
- Treatment Plan: A summary of the interventions implemented, including medication, therapy, lifestyle modifications, and other support services.
- Progress Notes: Detailed descriptions of the patient’s response to treatment, including any changes in symptoms, behaviors, or functional abilities.
- Goals and Objectives: Clearly defined, measurable, achievable, relevant, and time-bound (SMART) goals for the patient’s treatment.
- Plan for Next Visit: A summary of what the patient can expect at the next appointment, including any follow-up assessments or interventions.
Section 1: Detailed History and Assessment
This section is the foundation of the progress note, providing a comprehensive overview of the patient’s current state. It’s crucial to gather as much detail as possible, focusing on both the patient’s subjective experience and objective observations. A thorough HPI is essential for identifying patterns and potential triggers. For example, instead of simply stating “patient is anxious,” the note should detail the specific anxiety symptoms (e.g., racing heart, sweating, difficulty breathing), the context in which they occur, and the patient’s reported level of distress. The MSE should be meticulously documented, noting any specific behaviors or responses that are relevant to the patient’s condition. Consider using standardized assessment tools like the Beck Anxiety Inventory or the Hamilton Depression Rating Scale to quantify symptoms.
Section 2: Treatment Interventions and Response
This section details the interventions implemented and the patient’s response to them. It’s vital to document how the treatment is being delivered and the patient’s reaction to it. For example, if a patient is receiving medication, the note should describe the dosage, frequency, and any side effects experienced. If a therapy session is being conducted, the note should record the type of therapy, the goals of the session, and the patient’s engagement and progress. It’s important to track changes in symptoms, behaviors, and functional abilities. A key aspect of this section is to assess the patient’s adherence to treatment plans. Document any challenges encountered and the strategies used to address them. For instance, if a patient refuses medication, the note should document the reasons for the refusal and the clinician’s efforts to engage the patient in the process.

Section 3: Progress and Functional Status
This section focuses on the patient’s progress and functional status. It’s a critical area for monitoring the effectiveness of treatment and identifying areas for improvement. The note should include specific examples of the patient’s progress, noting any improvements in symptoms, behaviors, or functional abilities. For example, if a patient has made progress in managing their anxiety, the note should describe the specific strategies that have been effective and the patient’s reported level of comfort. It’s important to assess the patient’s ability to perform daily activities, such as self-care, work, or social engagement. This section should also include a rating of the patient’s functional status, using a standardized scale if appropriate. For example, the Functional Independence Scale (FI) can be used to assess the patient’s ability to perform activities of daily living.
Section 4: Challenges and Plan for Next Visit
This section acknowledges challenges encountered during the treatment process and outlines a plan for addressing them. It’s important to be honest and transparent about any difficulties that arise, and to document the steps taken to overcome them. For example, if a patient experiences a relapse of their symptoms, the note should describe the relapse, the interventions used to address it, and the patient’s response to the interventions. The plan for next visit should be specific and measurable, outlining the goals for the next appointment and the interventions that will be implemented. It’s crucial to collaborate with the patient to develop a plan that is tailored to their individual needs and preferences. Regularly reviewing the progress note is essential for ensuring continuity of care.
Section 5: Additional Considerations
Beyond the core sections, several additional considerations are important when documenting mental health care. Progress Note Template Mental Health should always be written in a clear, concise, and objective manner. Avoid using subjective language or making assumptions about the patient’s experience. Focus on factual observations and measurable data. Maintain a professional and empathetic tone. Ensure that the note is legible and easy to understand. Consider using standardized terminology and coding systems to improve the accuracy and consistency of the documentation. Finally, remember that the progress note is a tool for improving patient care, and it should be used to inform clinical decision-making and promote positive outcomes.

Conclusion
Effective progress note documentation is a cornerstone of quality mental health care. By utilizing a structured template and focusing on detailed observations, treatment interventions, and progress monitoring, healthcare providers can significantly enhance patient outcomes and improve the overall efficiency of the care process. The consistent application of this template, coupled with a commitment to clear and objective communication, contributes to a more responsive, collaborative, and ultimately, more effective healthcare system. Progress Note Template Mental Health is a vital tool for ensuring that patients receive the appropriate care they need to achieve their goals.
Conclusion
The comprehensive documentation of mental health care is not merely a bureaucratic exercise; it’s a critical element in promoting patient well-being and facilitating effective treatment. By utilizing a well-defined progress note template, healthcare professionals can effectively track patient progress, identify potential risks, and tailor interventions to meet individual needs. The consistent application of this template, coupled with a commitment to clear and objective communication, contributes to a more responsive, collaborative, and ultimately, more effective healthcare experience. Ultimately, prioritizing thorough and accurate documentation is an investment in the patient’s journey toward recovery and improved quality of life.
[ssba-buttons]