The neuro physical exam is a vital component of healthcare, providing a comprehensive assessment of a patient’s neurological function. It’s not just about identifying deficits; it’s about understanding the underlying causes and potential progression of neurological conditions. This template offers a structured approach to evaluating neurological function, allowing clinicians to tailor the assessment to the individual patient’s needs. A well-executed neuro physical exam can significantly impact diagnosis, treatment planning, and patient outcomes. This document provides a detailed guide to creating and utilizing a robust neuro physical exam template, ensuring consistent and reliable results. Neuro Physical Exam Template – understanding its components and proper application is crucial for effective patient care.
The initial step in creating a comprehensive neuro physical exam template involves careful planning and consideration of the patient’s specific clinical presentation and the suspected neurological condition. It’s important to remember that this is a dynamic process, and the assessment should be adjusted as new information becomes available. A thorough review of the patient’s medical history, including any previous neurological evaluations, is paramount. Furthermore, a clear understanding of the patient’s goals for the examination is essential – are they primarily focused on identifying deficits, assessing functional abilities, or exploring potential causes? This initial assessment will guide the selection of specific tests and the interpretation of results. The template should be adaptable to different patient populations and clinical scenarios.

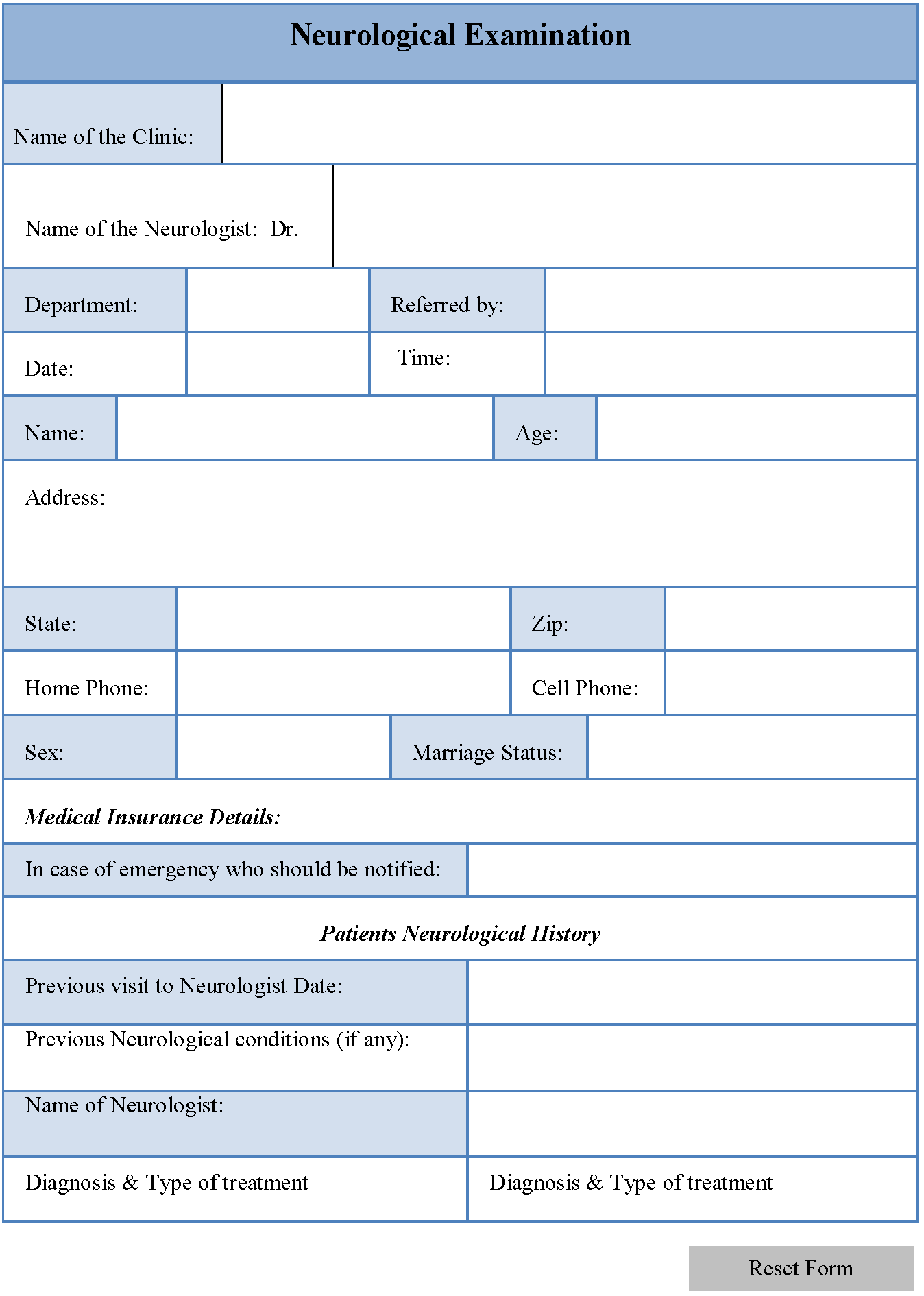
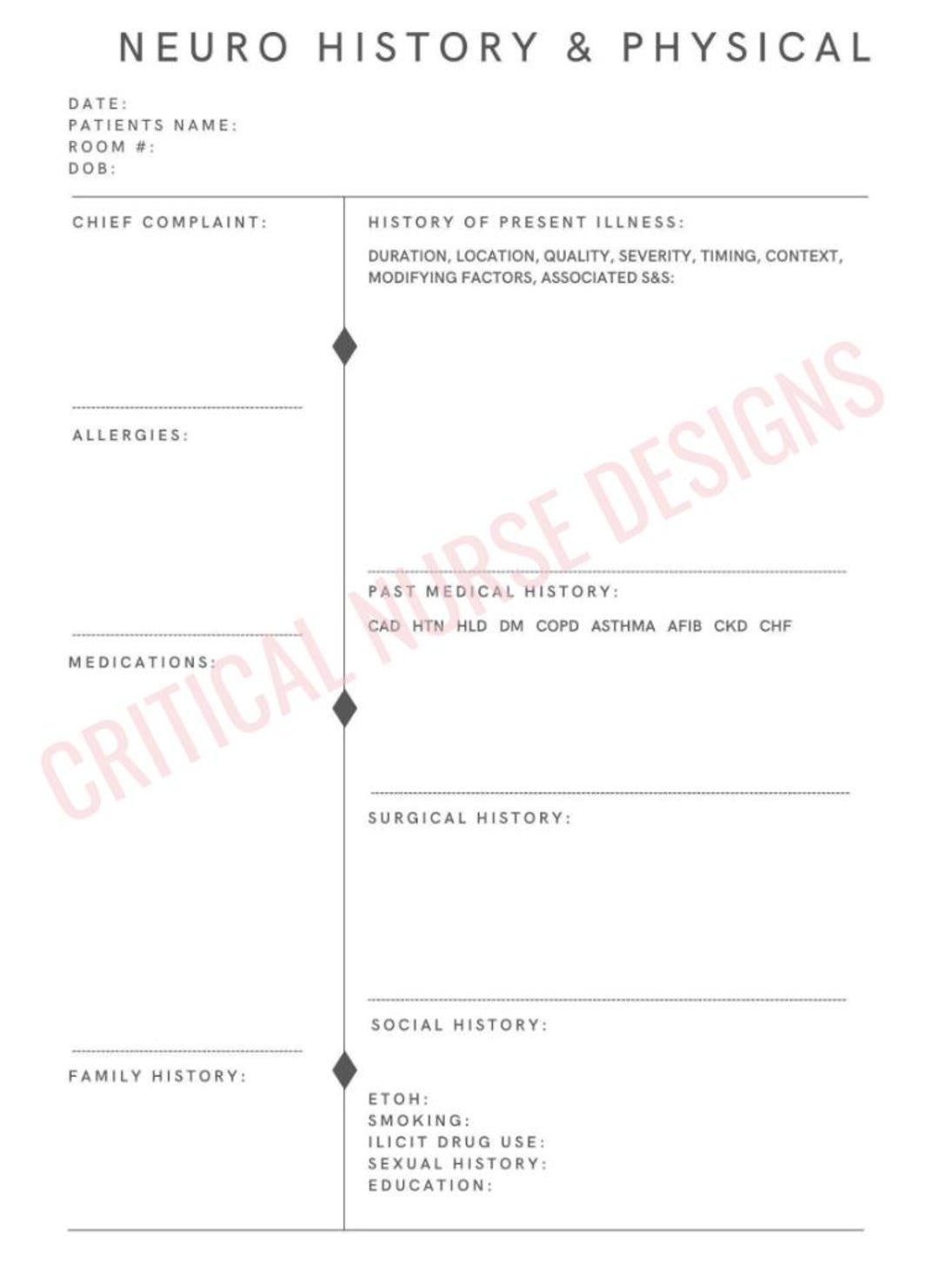
Section 1: Initial Assessment & Patient History
The first step in the neuro physical exam is always a thorough patient history. This section is critical for gathering information about the patient’s overall health, any relevant medical conditions, and any medications they are taking. Questions should explore symptoms, onset, duration, and severity of any neurological deficits. Specifically, clinicians should inquire about:
- Chief Complaint: What brings the patient in?
- Past Medical History: Any previous neurological conditions, surgeries, or hospitalizations?
- Medications: A complete list of all medications, including over-the-counter drugs and supplements.
- Social History: Smoking, alcohol use, and drug use – these can significantly impact neurological health.
- Family History: Any family history of neurological disorders?
Understanding the patient’s overall health status is fundamental to interpreting the neuro physical exam results. A detailed history allows the clinician to identify potential contributing factors and tailor the assessment accordingly. For example, a patient with a history of stroke may require a more focused assessment of motor function and cognitive abilities. The clinician should also inquire about any recent changes in the patient’s condition, such as increased pain, weakness, or sensory disturbances.
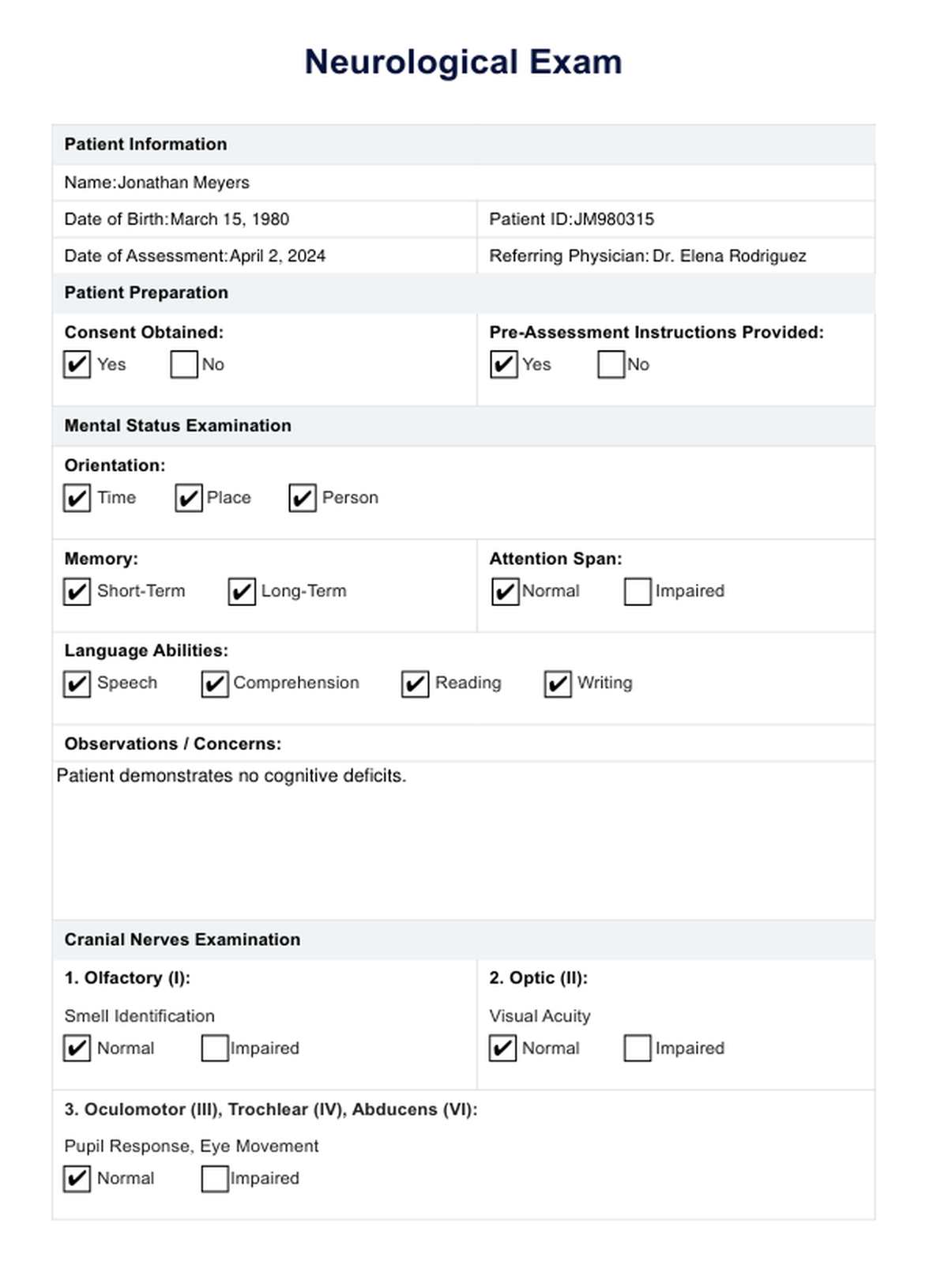
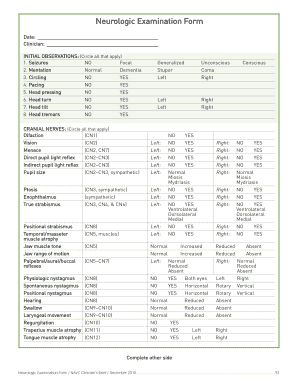
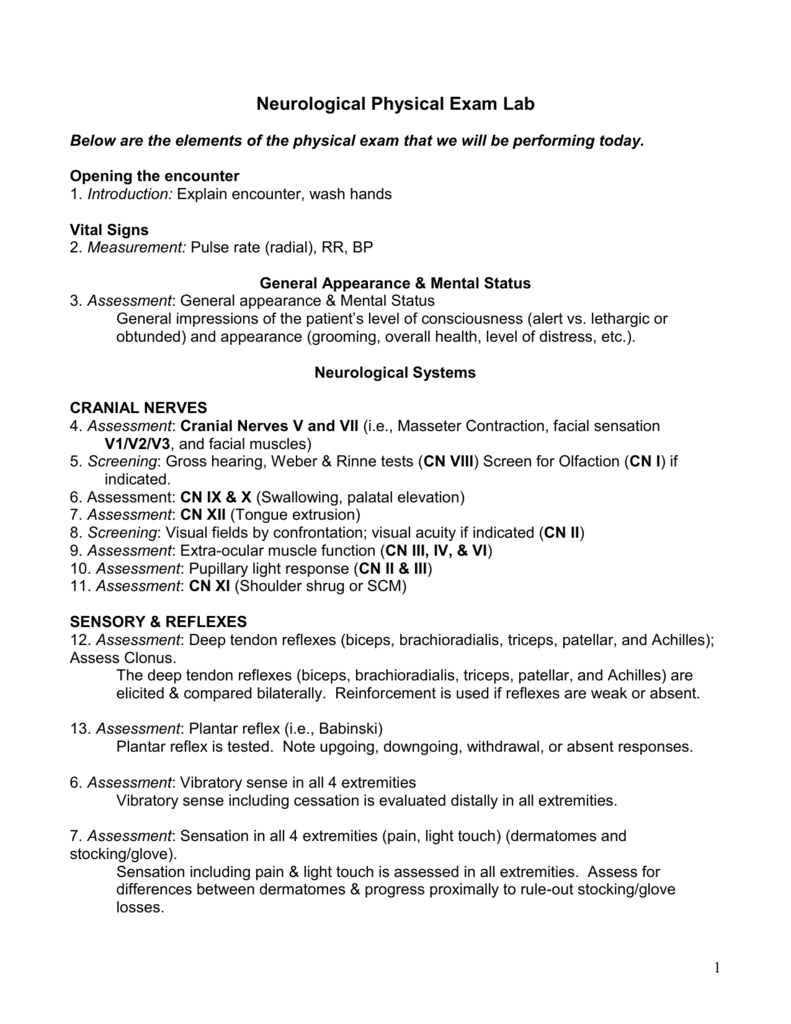
Section 2: Cranial Nerve Examination
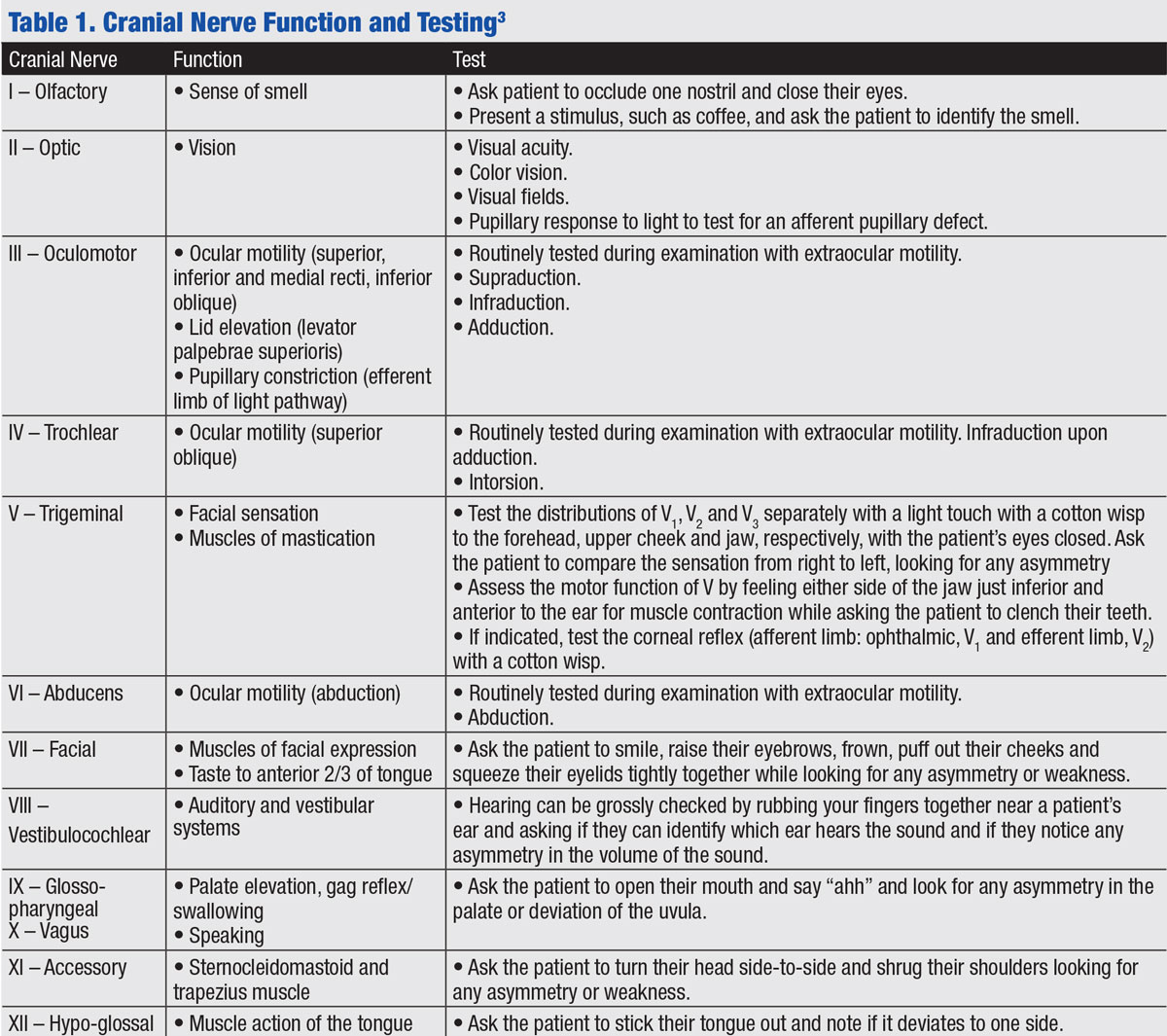
This section focuses on assessing the function of the cranial nerves. Each cranial nerve is responsible for transmitting sensory and motor information to and from the brain. A careful examination of each nerve is essential for identifying potential deficits.
- Olfactory Nerve (I): Assess for nasal congestion, decreased smell, and any signs of inflammation or infection.
- Optic Nerve (II): Evaluate for visual acuity, pupillary response, and any signs of optic disc edema or glaucoma.
- Oculomotor Nerve (III): Assess for pupillary reflexes, eye movements, and muscle strength of the eye muscles.
- Trochlear Nerve (IV): Evaluate for eye movements and pupillary reflexes.
- Trigeminal Nerve (V): Assess for facial sensation, mastication, and trigeminal neuralgia (painful trigeminal nerve stimulation).
- Abducens Nerve (VI): Evaluate for eye movements and assess for any signs of cranial nerve palsy.
- Facial Nerve (VII): Assess for facial sensation, taste, and facial expressions.
- Vestibulocochlear Nerve (VIII): Evaluate for hearing and balance.
The clinician should carefully observe the patient’s facial expressions, eye movements, and response to stimuli. Any deficits in these areas should be documented and correlated with the patient’s history. A thorough examination of the cranial nerves is crucial for identifying potential causes of neurological dysfunction.

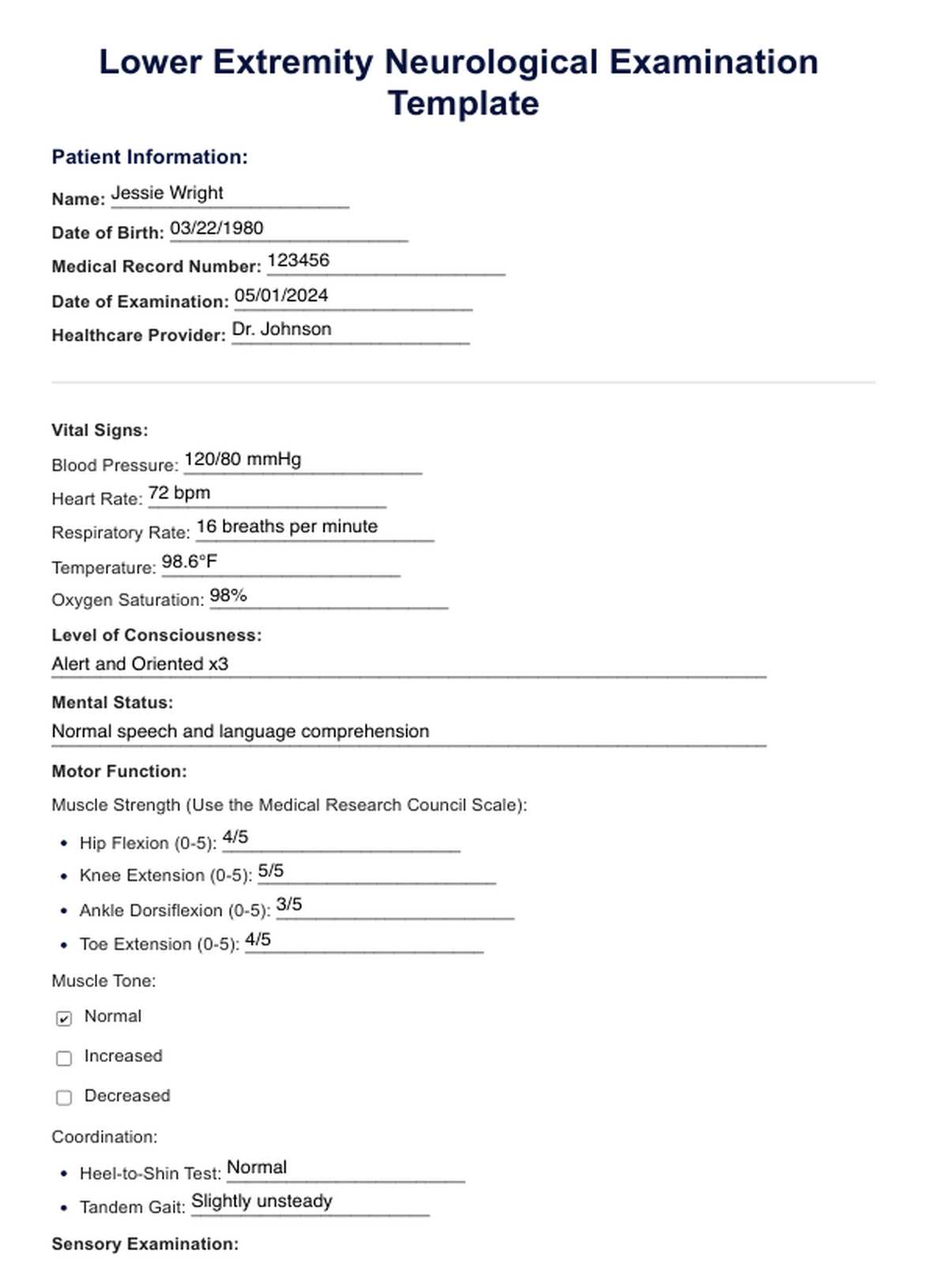
Section 3: Motor Function Assessment
This section assesses the patient’s ability to move their limbs and body. It’s important to consider the range of motion, strength, and coordination of each limb.

- Range of Motion (ROM): Assess the patient’s ability to move their joints through their full range of motion. This can be assessed using a manual muscle test (MMT) or a goniometer.
- Strength Testing: Perform strength tests to assess the strength of individual muscles. Common strength tests include the handgrip test, isometric testing, and dynamometry.
- Coordination and Balance: Assess the patient’s ability to coordinate their movements and maintain balance. This can be done using a balance test, such as the Romberg test or the single-leg stance test.
- Gait Analysis: Observe the patient’s walking pattern to identify any abnormalities, such as shuffling gait, reduced stride length, or difficulty with balance.
The clinician should carefully observe the patient’s movements and report any observed deficits. A detailed assessment of motor function is essential for identifying potential causes of neurological dysfunction, such as stroke, spinal cord injury, or peripheral neuropathy.
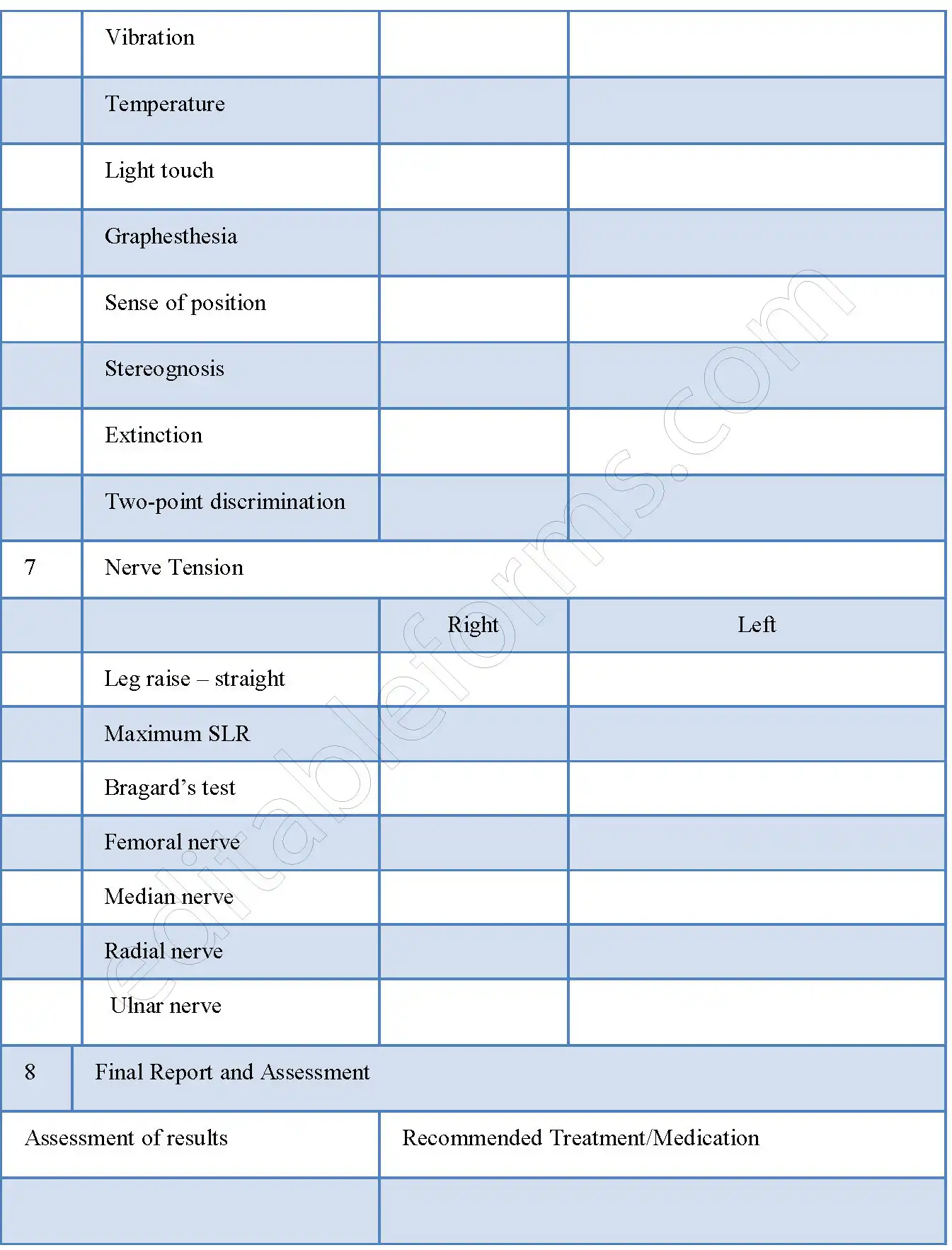
Section 4: Sensory Examination
This section assesses the patient’s ability to perceive sensations, including touch, pain, temperature, and vibration.
- Touch: Assess the patient’s response to touch, including the presence of pain, tingling, or numbness.
- Pain: Assess the patient’s pain levels using a pain scale (e.g., 0-10). Explore the patient’s history of pain, including the type of pain, location, and aggravating factors.
- Temperature: Assess the patient’s temperature perception.
- Vibration: Assess the patient’s response to vibration.
The clinician should carefully observe the patient’s response to stimuli and report any observed deficits. Sensory deficits can be a significant cause of neurological dysfunction, and it’s important to identify and address these deficits promptly.

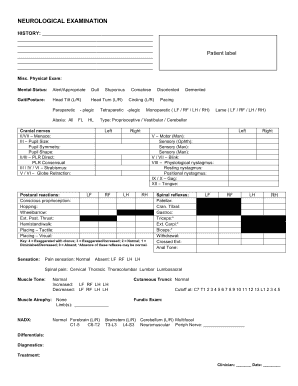
Section 5: Reflexes and Coordination
This section assesses the patient’s reflexes and coordination.
- Reflexes: Assess the patient’s reflexes to the extremities (e.g., knee-jerk reflex, ankle-jerk reflex). Assess the patient’s reflexes to the trunk (e.g., Babinski sign).
- Coordination: Assess the patient’s ability to coordinate their movements and maintain balance. This can be done using a tandem gait test or a timed reaction test.
The clinician should carefully observe the patient’s reflexes and coordination and report any observed abnormalities. Reflexes and coordination deficits can be a sign of neurological damage.
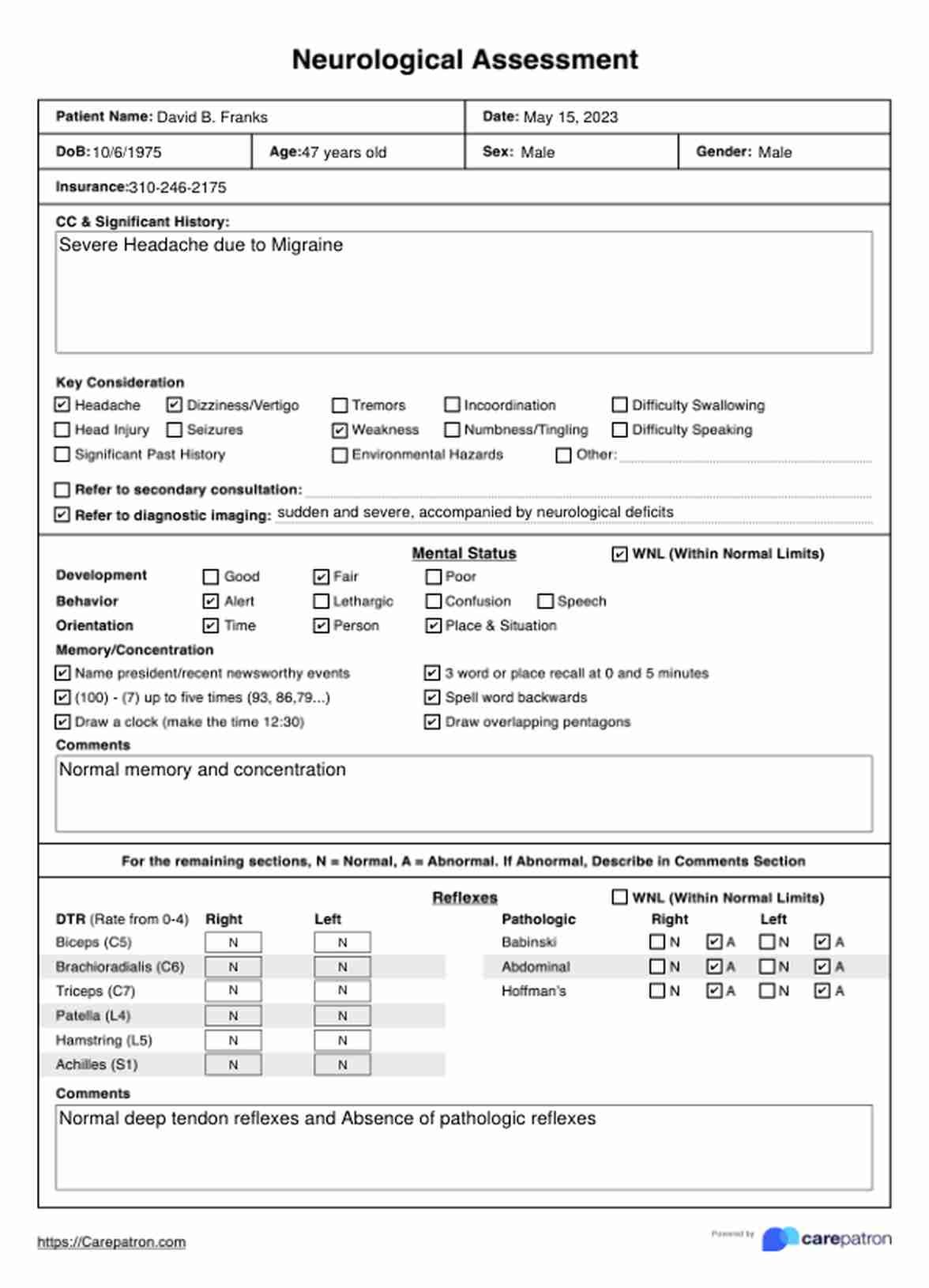
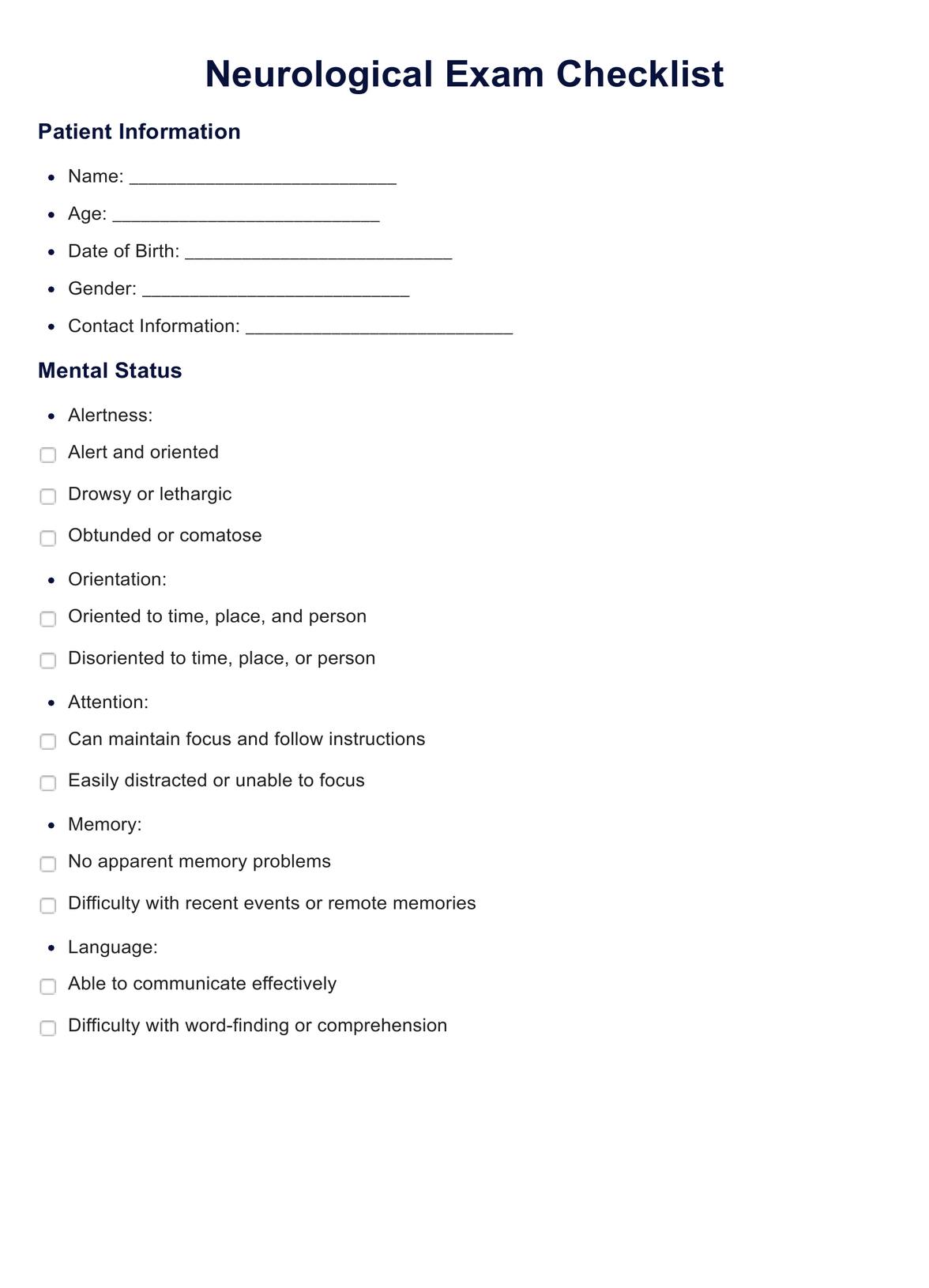
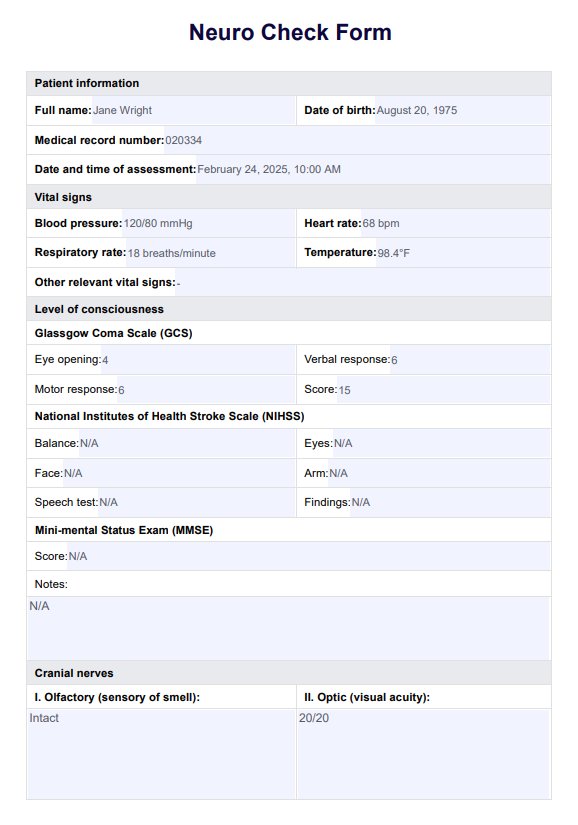
Section 6: Neurological Examination – General
This section provides a general overview of the patient’s neurological function, including mental status, orientation, and cranial nerve function.
- Mental Status: Assess the patient’s alertness, orientation, memory, and language.
- Orientation: Assess the patient’s awareness of their surroundings.
- Cranial Nerve Function: As described in Section 3, assess the function of the cranial nerves.
- Motor Function: Assess the patient’s motor function, including gait, balance, and coordination.
- Sensory Function: Assess the patient’s sensory function, including touch, pain, temperature, and vibration.
This section provides a broad overview of the patient’s neurological function and helps to identify any potential neurological deficits.
Conclusion
The neuro physical exam template provides a structured framework for evaluating neurological function. By systematically assessing various neurological domains, clinicians can gain a comprehensive understanding of a patient’s neurological condition and develop an appropriate treatment plan. Regular and thorough neuro physical exams are essential for monitoring the progression of neurological deficits and ensuring optimal patient outcomes. Remember that this template is a guide, and the clinician should always adapt the assessment to the individual patient’s needs and clinical presentation. Neuro Physical Exam Template – consistent application of this template is key to accurate diagnosis and effective patient care.
Conclusion
The neuro physical exam is a cornerstone of neurological assessment, providing a vital tool for clinicians to understand the patient’s neurological status. By utilizing a well-defined template and carefully considering the patient’s individual needs, clinicians can generate accurate and reliable results, ultimately contributing to improved patient care and outcomes. The continued refinement and adaptation of the neuro physical exam template based on advancements in neuroimaging and diagnostic techniques will undoubtedly enhance its effectiveness in the future. Ultimately, a thorough and systematic neuro physical exam empowers clinicians to provide the best possible care for patients with neurological conditions.
[ssba-buttons]